Amlodipine besylate, valsartan, hydrochlorothiazide.
Each film-coated tablet contains 5 mg of amlodipine (as amlodipine besylate), 160 mg of valsartan and 12.5 mg of hydrochlorothiazide.
Each film-coated tablet contains 10 mg of amlodipine (as amlodipine besylate), 160 mg of valsartan and 12.5 mg of hydrochlorothiazide.
Each film-coated tablet contains 10 mg of amlodipine (as amlodipine besylate), 160 mg of valsartan and 25 mg of hydrochlorothiazide.
Excipients/Inactive Ingredients: Tablet core: Cellulose microcrystalline, Crospovidone, Colloidal anhydrous silica, Magnesium stearate.
Coating (Exforge HCT 5 mg/160 mg/12.5 mg film-coated tablets): Hypromellose, Macrogol 4000, Talc, Titanium dioxide (E171).
Coating (Exforge HCT 10 mg/160 mg/12.5 mg film-coated tablets): Hypromellose, Macrogol 4000, Talc, Titanium dioxide (E171), Yellow iron oxide (E172) Red iron oxide (E172).
Coating (Exforge HCT 10 mg/160 mg/25 mg film-coated tablets): Hypromellose, Macrogol 4000, Talc, Yellow iron oxide (E172).
Pharmacotherapeutic group: Agents acting on the renin-angiotensin system, angiotensin II antagonists, other combinations. ATC code: C09DX01.
Pharmacology: Pharmacodynamics: Mechanism of action: Exforge HCT combines three antihypertensive compounds with complementary mechanisms to control blood pressure in patients with essential hypertension: amlodipine belongs to the calcium antagonist class and valsartan to the angiotensin II antagonist class of medicines and hydrochlorothiazide belongs to the thiazide diuretics class of medicines. The combination of these substances has an additive antihypertensive effect.
Amlodipine/Valsartan/Hydrochlorothiazide: Clinical efficacy and safety: Exforge HCT was studied in a double-blind, active controlled study in hypertensive patients. A total of 2,271 patients with moderate to severe hypertension (mean baseline systolic/diastolic blood pressure was 170/107 mmHg) received treatments of amlodipine/valsartan/hydrochlorothiazide 10 mg/320 mg/25 mg, valsartan/hydrochlorothiazide 320 mg/25 mg, amlodipine/valsartan 10 mg/320 mg, or hydrochlorothiazide/amlodipine 25 mg/10 mg. At study initiation patients were assigned lower doses of their treatment combination and were titrated to their full treatment dose by week 2.
At week 8, the mean reductions in systolic/diastolic blood pressure were 39.7/24.7 mmHg with Exforge HCT, 32.0/19.7 mmHg with valsartan/hydrochlorothiazide, 33.5/21.5 mmHg with amlodipine/valsartan, and 31.5/19.5 mmHg with amlodipine/hydrochlorothiazide. The triple combination therapy was statistically superior to each of the three dual combination treatments in reduction of diastolic and systolic blood pressures. The reductions in systolic/diastolic blood pressure with Exforge HCT were 7.6/5.0 mmHg greater than with valsartan/hydrochlorothiazide, 6.2/3.3 mmHg greater than with amlodipine/valsartan, and 8.2/5.3 mmHg greater than with amlodipine/hydrochlorothiazide. The full blood pressure lowering effect was achieved 2 weeks after being on their maximal dose of Exforge HCT. Statistically greater proportions of patients achieved blood pressure control (<140/90 mmHg) with Exforge HCT (71%) compared to each of the three dual combination therapies (45-54%) (p<0.0001).
In a subgroup of 283 patients focusing on ambulatory blood pressure monitoring, clinically and statistically superior reductions in 24-hour systolic and diastolic blood pressures were observed with the triple combination compared to valsartan/hydrochlorothiazide, valsartan/amlodipine, and hydrochlorothiazide/amlodipine.
Amlodipine: Mechanism of action: The amlodipine component of Exforge HCT inhibits the transmembrane entry of calcium ions into cardiac and vascular smooth muscle. The mechanism of the antihypertensive action of amlodipine is due to a direct relaxant effect on vascular smooth muscle, causing reductions in peripheral vascular resistance and in blood pressure.
Pharmacodynamic effects: Experimental data suggest that amlodipine binds to both dihydropyridine and non-dihydropyridine binding sites. The contractile processes of cardiac muscle and vascular smooth muscle are dependent upon the movement of extracellular calcium ions into these cells through specific ion channels.
Following administration of therapeutic doses to patients with hypertension, amlodipine produces vasodilation, resulting in a reduction of supine and standing blood pressures. These decreases in blood pressure are not accompanied by a significant change in heart rate or plasma catecholamine levels with chronic dosing.
Plasma concentrations correlate with effect in both young and elderly patients.
In hypertensive patients with normal renal function, therapeutic doses of amlodipine resulted in a decrease in renal vascular resistance and increases in glomerular filtration rate and effective renal plasma flow, without change in filtration fraction or proteinuria.
As with other calcium channel blockers, haemodynamic measurements of cardiac function at rest and during exercise (or pacing) in patients with normal ventricular function treated with amlodipine have generally demonstrated a small increase in cardiac index without significant influence on dP/dt or on left ventricular end diastolic pressure or volume. In haemodynamic studies, amlodipine has not been associated with a negative inotropic effect when administered in the therapeutic dose range to intact animals and humans, even when co-administered with beta blockers to humans.
Amlodipine does not change sinoatrial nodal function or atrioventricular conduction in intact animals or humans. In clinical studies in which amlodipine was administered in combination with beta blockers to patients with either hypertension or angina, no adverse effects on electrocardiographic parameters were observed.
Amlodipine has been studied in patients with chronic stable angina, vasospastic angina and angiographically documented coronary artery disease.
Clinical efficacy and safety: Use in patients with hypertension: A randomised double-blind morbidity-mortality study called the Antihypertensive and Lipid-Lowering treatment to prevent Heart Attack Trial (ALLHAT) was performed to compare newer therapies: amlodipine 2.5-10 mg/day (calcium channel blocker) or lisinopril 10-40 mg/day (ACE-inhibitor) as first-line therapies to that of the thiazide-diuretic, chlorthalidone 12.5-25 mg/day in mild to moderate hypertension.
A total of 33,357 hypertensive patients aged 55 or older were randomised and followed for a mean of 4.9 years. The patients had at least one additional coronary heart disease risk factor, including: previous myocardial infarction or stroke (>6 months prior to enrollment) or documentation of other atherosclerotic cardiovascular disease (overall 51.5%), type 2 diabetes (36.1%), high density lipoprotein - cholesterol <35 mg/dl or <0.906 mmol/l (11.6%), left ventricular hypertrophy diagnosed by electrocardiogram or echocardiography (20.9%), current cigarette smoking (21.9%).
The primary endpoint was a composite of fatal coronary heart disease or non-fatal myocardial infarction. There was no significant difference in the primary endpoint between amlodipine-based therapy and chlorthalidone-based therapy: risk ratio (RR) 0.98 95% CI (0.90-1.07) p=0.65. Among secondary endpoints, the incidence of heart failure (component of a composite combined cardiovascular endpoint) was significantly higher in the amlodipine group as compared to the chlorthalidone group (10.2% versus 7.7%, RR 1.38, 95% CI [1.25-1.52] p<0.001). However, there was no significant difference in all-cause mortality between amlodipine-based therapy and chlorthalidone-based therapy RR 0.96 95% CI [0.89-1.02] p=0.20.
Valsartan: Mechanism of action: Valsartan is an orally active, potent and specific angiotensin II receptor antagonist. It acts selectively on the receptor subtype AT1, which is responsible for the known actions of angiotensin II.
Clinical efficacy and safety: Administration of valsartan to patients with hypertension results in a drop in blood pressure without affecting pulse rate.
In most patients, after administration of a single oral dose, onset of antihypertensive activity occurs within 2 hours, and the peak drop in blood pressure is achieved within 4-6 hours. The antihypertensive effect persists over 24 hours after administration. During repeated administration, the maximum reduction in blood pressure with any dose is generally attained within 2-4 weeks.
Hydrochlorothiazide: Mechanism of action: The site of action of thiazide diuretics is primarily in the renal distal convoluted tubule. It has been shown that there is a high-affinity receptor in the renal cortex as the primary binding site for the thiazide diuretic action and inhibition of NaCl transport in the distal convoluted tubule. The mode of action of thiazides is through inhibition of the Na+Cl- symporter perhaps by competing for the Cl- site, thereby affecting electrolyte reabsorption mechanisms: directly increasing sodium and chloride excretion to an approximately equal extent, and indirectly, by this diuretic action, reducing plasma volume, with consequent increases in plasma renin activity, aldosterone secretion and urinary potassium loss, and a decrease in serum potassium.
Non-melanoma skin cancer: Based on available data from epidemiological studies, cumulative dose dependent association between hydrochlorothiazide and NMSC has been observed. One study included a population comprised of 71,533 cases of BCC and of 8,629 cases of SCC matched to 1,430,833 and 172,462 population controls, respectively. High hydrochlorothiazide use (≥50000 mg cumulative) was associated with an adjusted odds ratio (OR) of 1.29 (95% CI: 1.23-1.35) for BCC and 3.98 (95% CI: 3.68-4.31) for SCC. A clear cumulative dose response relationship was observed for both BCC and SCC. Another study showed a possible association between lip cancer (SCC) and exposure to hydrochlorothiazide: 633 cases of lip cancer were matched with 63,067 population controls, using a risk-set sampling strategy. A cumulative dose-response relationship was demonstrated with an adjusted OR 2.1 (95% CI: 1.7-2.6) increasing to OR 3.9 (3.0-4.9) for high use (~25000 mg) and OR 7.7 (5.7-10.5) for the highest cumulative dose (~100000 mg) (see also Precautions).
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with Exforge HCT in all subsets of the paediatric population in essential hypertension. See Dosage & Administration for information on paediatric use.
Other: dual blockade of the renin-angiotensin-aldosterone system (RAAS): Two large randomised, controlled trials (ONTARGET [ONgoing Telmisartan Alone and in combination with Ramipril Global Endpoint Trial] and VA NEPHRON-D [The Veterans Affairs Nephropathy in Diabetes]) have examined the use of the combination of an ACE inhibitor with an ARB.
ONTARGET was a study conducted in patients with a history of cardiovascular or cerebrovascular disease, or type 2 diabetes mellitus accompanied by evidence of end-organ damage. VA NEPHRON-D was a study in patients with type 2 diabetes mellitus and diabetic nephropathy.
These studies have shown no significant beneficial effect on renal and/or cardiovascular outcomes and mortality, while an increased risk of hyperkalaemia, acute kidney injury and/or hypotension as compared to monotherapy was observed. Given their similar pharmacodynamic properties, these results are also relevant for other ACE inhibitors and ARBs.
ACE inhibitors and ARBs should therefore not be used concomitantly in patients with diabetic nephropathy (see Precautions).
ALTITUDE (Aliskiren Trial in Type 2 Diabetes Using Cardiovascular and Renal Disease Endpoints) was a study designed to test the benefit of adding aliskiren to a standard therapy of an ACE inhibitor or an ARB in patients with type 2 diabetes mellitus and chronic kidney disease, cardiovascular disease, or both. The study was terminated early because of an increased risk of adverse outcomes. Cardiovascular death and stroke were both numerically more frequent in the aliskiren group than in the placebo group and adverse events and serious adverse events of interest (hyperkalaemia, hypotension and renal dysfunction) were more frequently reported in the aliskiren group than in the placebo group.
Pharmacokinetics: Linearity: Amlodipine, valsartan and hydrochlorothiazide exhibit linear pharmacokinetics.
Amlodipine/valsartan/hydrochlorothiazide: Following oral administration of Exforge HCT in normal healthy adults, peak plasma concentrations of amlodipine, valsartan and hydrochlorothiazide are reached in 6-8 hours, 3 hours, and 2 hours, respectively. The rate and extent of absorption of amlodipine, valsartan and hydrochlorothiazide from Exforge HCT are the same as when administered as individual dosage forms.
Amlodipine: Absorption: After oral administration of therapeutic doses of amlodipine alone, peak plasma concentrations of amlodipine are reached in 6-12 hours. Absolute bioavailability has been calculated as between 64% and 80%. Amlodipine bioavailability is unaffected by food ingestion.
Distribution: Volume of distribution is approximately 21 l/kg. In vitro studies with amlodipine have shown that approximately 97.5% of circulating drug is bound to plasma proteins.
Biotransformation: Amlodipine is extensively (approximately 90%) metabolised in the liver to inactive metabolites.
Elimination: Amlodipine elimination from plasma is biphasic, with a terminal elimination half-life of approximately 30 to 50 hours. Steady-state plasma levels are reached after continuous administration for 7-8 days. Ten per cent of original amlodipine and 60% of amlodipine metabolites are excreted in urine.
Valsartan: Absorption: Following oral administration of valsartan alone, peak plasma concentrations of valsartan are reached in 2-4 hours. Mean absolute bioavailability is 23%. Food decreases exposure (as measured by AUC) to valsartan by about 40% and peak plasma concentration (Cmax) by about 50%, although from about 8 h post dosing plasma valsartan concentrations are similar for the fed and fasted groups. This reduction in AUC is not, however, accompanied by a clinically significant reduction in the therapeutic effect, and valsartan can therefore be given either with or without food.
Distribution: The steady-state volume of distribution of valsartan after intravenous administration is about 17 litres, indicating that valsartan does not distribute into tissues extensively. Valsartan is highly bound to serum proteins (94-97%), mainly serum albumin.
Biotransformation: Valsartan is not transformed to a high extent as only about 20% of dose is recovered as metabolites. A hydroxy metabolite has been identified in plasma at low concentrations (less than 10% of the valsartan AUC). This metabolite is pharmacologically inactive.
Elimination: Valsartan shows multiexponential decay kinetics (t½α <1 h and t½β about 9 h). Valsartan is primarily eliminated in faeces (about 83% of dose) and urine (about 13% of dose), mainly as unchanged drug. Following intravenous administration, plasma clearance of valsartan is about 2 l/h and its renal clearance is 0.62 l/h (about 30% of total clearance). The half-life of valsartan is 6 hours.
Hydrochlorothiazide: Absorption: The absorption of hydrochlorothiazide, after an oral dose, is rapid (Tmax about 2 hours). The increase in mean AUC is linear and dose proportional in the therapeutic range.
The effect of food on hydrochlorothiazide absorption, if any, has little clinical significance. Absolute bioavailability of hydrochlorothiazide is 70% after oral administration.
Distribution: The apparent volume of distribution is 4-8 l/kg. Circulating hydrochlorothiazide is bound to serum proteins (40-70%), mainly serum albumin. Hydrochlorothiazide also accumulates in erythrocytes at approximately 3 times the level in plasma.
Biotransformation: Hydrochlorothiazide is eliminated predominantly as unchanged compound.
Elimination: Hydrochlorothiazide is eliminated from plasma with a half-life averaging 6 to 15 hours in the terminal elimination phase. There is no change in the kinetics of hydrochlorothiazide on repeated dosing, and accumulation is minimal when dosed once daily. More than 95% of the absorbed dose is being excreted as unchanged compound in the urine. The renal clearance is composed of passive filtration and active secretion into the renal tubule.
Special populations: Paediatric patients (age below 18 years): No pharmacokinetic data are available in the paediatric population.
Elderly (age 65 years or over): Time to peak plasma amlodipine concentrations is similar in young and elderly patients. In elderly patients, amlodipine clearance tends to decline, causing increases in the area under the curve (AUC) and elimination half-life. Mean systemic AUC of valsartan is higher by 70% in the elderly than in the young, therefore caution is required when increasing the dosage.
Systemic exposure to valsartan is slightly elevated in the elderly as compared to the young, but this has not been shown to have any clinical significance.
Limited data suggest that the systemic clearance of hydrochlorothiazide is reduced in both healthy and hypertensive elderly subjects compared to young healthy volunteers.
Since the three components are equally well tolerated in younger and elderly patients, normal dose regimens are recommended (see Dosage & Administration).
Renal impairment: The pharmacokinetics of amlodipine are not significantly influenced by renal impairment. As expected for a compound where renal clearance accounts for only 30% of total plasma clearance, no correlation was seen between renal function and systemic exposure to valsartan.
Patients with mild to moderate renal impairment may therefore receive the usual initial dose (see Dosage & Administration and Precautions).
In the presence of renal impairment, mean peak plasma levels and AUC values of hydrochlorothiazide are increased and the urinary excretion rate is reduced. In patients with mild to moderate renal impairment, a 3-fold increase in hydrochlorothiazide AUC has been observed. In patients with severe renal impairment an 8-fold increase in AUC has been observed. Exforge HCT is contraindicated in patients with severe renal impairment, anuria or undergoing dialysis (see Contraindications).
Hepatic impairment: Very limited clinical data are available regarding amlodipine administration in patients with hepatic impairment. Patients with hepatic impairment have decreased clearance of amlodipine with resulting increase of approximately 40-60% in AUC. On average, in patients with mild to moderate chronic liver disease, exposure (measured by AUC values) to valsartan is twice that found in healthy volunteers (matched by age, sex and weight). Due to the valsartan component, Exforge HCT is contraindicated in patients with hepatic impairment (see Dosage & Administration and Contraindications).
Toxicology: Preclinical safety data: Amlodipine/Valsartan/Hydrochlorothiazide: In a variety of preclinical safety studies conducted in several animal species with amlodipine, valsartan, hydrochlorothiazide, valsartan/hydrochlorothiazide, amlodipine/valsartan and amlodipine/valsartan/hydrochlorothiazide (Exforge HCT), there was no evidence of systemic or target organ toxicity that would adversely affect the development of Exforge HCT for clinical use in humans.
Preclinical safety studies of up to 13 weeks in duration were conducted with amlodipine/valsartan/hydrochlorothiazide in rats. The combination resulted in expected reduction of red blood cell mass (erythrocytes, haemoglobin, haematocrit, and reticulocytes), increase in serum urea, increase in serum creatinine, increase in serum potassium, juxtaglomerular (JG) hyperplasia in the kidney and focal erosions in the glandular stomach in rats. All these changes were reversible after a 4-week recovery period and were considered to be exaggerated pharmacological effects.
The amlodipine/valsartan/hydrochlorothiazide combination was not tested for genotoxicity or carcinogenicity as there was no evidence of any interaction between these substances, which have been on the market for a long time. However, amlodipine, valsartan and hydrochlorothiazide have been tested individually for genotoxicity and carcinogenicity with negative results.
Amlodipine: Reproductive toxicology: Reproductive studies in rats and mice have shown delayed date of delivery, prolonged duration of labour and decreased pup survival at dosages approximately 50 times greater than the maximum recommended dosage for humans based on mg/kg.
Impairment of fertility: There was no effect on the fertility of rats treated with amlodipine (males for 64 days and females 14 days prior to mating) at doses up to 10 mg/kg/day (8 times* the maximum recommended human dose of 10 mg on a mg/m2 basis). In another rat study in which male rats were treated with amlodipine besilate for 30 days at a dose comparable with the human dose based on mg/kg, decreased plasma follicle-stimulating hormone and testosterone were found as well as decreases in sperm density and in the number of mature spermatids and Sertoli cells.
Carcinogenesis, mutagenesis: Rats and mice treated with amlodipine in the diet for two years, at concentrations calculated to provide daily dosage levels of 0.5, 1.25, and 2.5 mg/kg/day showed no evidence of carcinogenicity. The highest dose (for mice, similar to, and for rats twice* the maximum recommended clinical dose of 10 mg on a mg/m2 basis) was close to the maximum tolerated dose for mice but not for rats.
Mutagenicity studies revealed no drug related effects at either the gene or chromosome levels.
* Based on patient weight of 50 kg.
Valsartan: Non-clinical data reveal no special hazard for humans based on conventional studies of safety pharmacology, repeated dose toxicity, genotoxicity, carcinogenic potential, toxicity to reproduction and development.
In rats, maternally toxic doses (600 mg/kg/day) during the last days of gestation and lactation led to lower survival, lower weight gain and delayed development (pinna detachment and ear-canal opening) in the offspring (see Use in Pregnancy & Lactation). These doses in rats (600 mg/kg/day) are approximately 18 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient).
In non-clinical safety studies, high doses of valsartan (200 to 600 mg/kg body weight) caused in rats a reduction of red blood cell parameters (erythrocytes, haemoglobin, haematocrit) and evidence of changes in renal haemodynamics (slightly raised blood urea nitrogen, and renal tubular hyperplasia and basophilia in males). These doses in rats (200 and 600 mg/kg/day) are approximately 6 and 18 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient).
In marmosets at comparable doses, the changes were similar though more severe, particularly in the kidney where the changes developed to a nephropathy including raised blood urea nitrogen and creatinine.
Hypertrophy of the renal juxtaglomerular cells was also seen in both species. All changes were considered to be caused by the pharmacological action of valsartan which produces prolonged hypotension, particularly in marmosets. For therapeutic doses of valsartan in humans, the hypertrophy of the renal juxtaglomerular cells does not seem to have any relevance.
Treatment of essential hypertension as substitution therapy in adult patients whose blood pressure is adequately controlled on the combination of amlodipine, valsartan and hydrochlorothiazide (HCT), taken either as three single-component formulations or as a dual-component and a single-component formulation.
Posology: The recommended dose of Exforge HCT is one tablet per day, to be taken preferably in the morning.
Before switching to Exforge HCT patients should be controlled on stable doses of the monocomponents taken at the same time. The dose of Exforge HCT should be based on the doses of the individual components of the combination at the time of switching.
The maximum recommended dose of Exforge HCT is 10 mg/320 mg/25 mg.
Special populations: Renal impairment: Due to the hydrochlorothiazide component, Exforge HCT is contraindicated for use in patients with anuria (see Contraindications) and in patients with severe renal impairment (glomerular filtration rate (GFR) <30 ml/min/1.73 m2) (see Contraindications, Precautions and Pharmacology: Pharmacokinetics under Actions).
No adjustment of the initial dose is required for patients with mild to moderate renal impairment (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Hepatic impairment: Due to the valsartan component, Exforge HCT is contraindicated in patients with severe hepatic impairment (see Contraindications). In patients with mild to moderate hepatic impairment without cholestasis, the maximum recommended dose is 80 mg valsartan and therefore Exforge HCT is not suitable in this group of patients (see Contraindications, Precautions and Pharmacology: Pharmacokinetics under Actions). Amlodipine dosage recommendations have not been established in patients with mild to moderate hepatic impairment. When switching eligible hypertensive patients (see Indications/Uses) with hepatic impairment to Exforge HCT, the lowest available dose of the amlodipine component should be used.
Heart failure and coronary artery disease: There is limited experience with the use of Exforge HCT, particulary at the maximum dose, in patients with heart failure and coronary artery disease. Caution is advised in patients with heart failure and coronary artery disease, particularly at the maximum dose of Exforge HCT, 10 mg/320 mg/25 mg.
Elderly (age 65 years or over): Caution, including more frequent monitoring of blood pressure, is recommended in elderly patients, particularly at the maximum dose of Exforge HCT, 10 mg/320 mg/25 mg, since available data in this patient population are limited. When switching eligible elderly hypertensive patients (see Indications/Uses) to Exforge HCT, the lowest available dose of the amlodipine component should be used.
Paediatric population: There is no relevant use of Exforge HCT in the paediatric population (patients below age 18 years) for the indication of essential hypertension.
Method of administration: Exforge HCT can be taken with or without food. The tablets should be swallowed whole with some water, at the same time of the day and preferably in the morning.
Symptoms: There is no experience of overdose with Exforge HCT. The major symptom of overdose with valsartan is possibly pronounced hypotension with dizziness. Overdose with amlodipine may result in excessive peripheral vasodilation and, possibly, reflex tachycardia. Marked and potentially prolonged systemic hypotension, including shock with fatal outcome, have been reported with amlodipine.
Treatment: Amlodipine/Valsartan/Hydrochlorothiazide: Clinically significant hypotension due to Exforge HCT overdose calls for active cardiovascular support, including frequent monitoring of cardiac and respiratory function, elevation of extremities and attention to circulating fluid volume and urine output. A vasoconstrictor may be helpful in restoring vascular tone and blood pressure, provided that there is no contraindication to its use. Intravenous calcium gluconate may be beneficial in reversing the effects of calcium channel blockade.
Amlodipine: If ingestion is recent, induction of vomiting or gastric lavage may be considered. Administration of activated charcoal to healthy volunteers immediately or up to two hours after ingestion of amlodipine has been shown to significantly decrease amlodipine absorption.
Amlodipine is unlikely to be removed by haemodialysis.
Valsartan: Valsartan is unlikely to be removed by haemodialysis.
Hydrochlorothiazide: Overdose with hydrochlorothiazide is associated with electrolyte depletion (hypokalaemia, hypochloraemia) and hypovolaemia resulting from excessive diuresis. The most common signs and symptoms of overdose are nausea and somnolence. Hypokalaemia may result in muscle spasms and or accentuate arrhythmia associated with the concomitant use of digitalis glycosides or certain anti-arrhythmic medicinal products.
The degree to which hydrochlorothiazide is removed by haemodialysis has not been established.
Hypersensitivity to the active substances, to other sulphonamide derivatives, to dihydropyridine derivatives, or to any of the excipients.
Second and third trimesters of pregnancy (see Precautions and Use in Pregnancy & Lactation).
Hepatic impairment, biliary cirrhosis or cholestasis.
Severe renal impairment (GFR <30 ml/min/1.73 m2), anuria and patients undergoing dialysis.
Concomitant use of Exforge HCT with aliskiren-containing products in patients with diabetes mellitus or renal impairment (GFR <60 ml/min/1.73 m2) (see Precautions and Interactions).
Refractory hypokalaemia, hyponatraemia, hypercalcaemia, and symptomatic hyperuricaemia.
Severe hypotension.
Shock (including cardiogenic shock).
Obstruction of the outflow tract of the left ventricle (e.g. hypertrophic obstructive cardiomyopathy and high grade aortic stenosis).
Haemodynamically unstable heart failure after acute myocardial infarction.
The safety and efficacy of amlodipine in hypertensive crisis have not been established.
Sodium- and/or volume-depleted patients: Excessive hypotension, including orthostatic hypotension, was seen in 1.7% of patients treated with the maximum dose of Exforge HCT (10 mg/320 mg/25 mg) compared to 1.8% of valsartan/hydrochlorothiazide (320 mg/25 mg) patients, 0.4% of amlodipine/valsartan (10 mg/320 mg) patients, and 0.2% of hydrochlorothiazide/amlodipine (25 mg/10 mg) patients in a controlled trial in patients with moderate to severe uncomplicated hypertension.
In sodium-depleted and/or volume-depleted patients, such as those receiving high doses of diuretics, symptomatic hypotension may occur after initiation of treatment with Exforge HCT. Exforge HCT should be used only after correction of any pre-existing sodium and/or volume depletion.
If excessive hypotension occurs with Exforge HCT, the patient should be placed in the supine position and, if necessary, given an intravenous infusion of normal saline. Treatment can be continued once blood pressure has been stabilised.
Serum electrolyte changes: Amlodipine/valsartan/hydrochlorothiazide: In the controlled trial of Exforge HCT, the counteracting effects of valsartan 320 mg and hydrochlorothiazide 25 mg on serum potassium approximately balanced each other in many patients. In other patients, one or the other effect may be dominant. Periodic determinations of serum electrolytes to detect possible electrolyte imbalance should be performed at appropriate intervals.
Periodic determination of serum electrolytes and potassium in particular should be performed at appropriate intervals to detect possible electrolyte imbalance, especially in patients with other risk factors such as impaired renal function, treatment with other medicinal products or history of prior electrolyte imbalances.
Valsartan: Concomitant use with potassium supplements, potassium-sparing diuretics, salt substitutes containing potassium, or other medicinal products that may increase potassium levels (heparin, etc.) is not recommended. Monitoring of potassium should be undertaken as appropriate.
Hydrochlorothiazide: Treatment with Exforge HCT should only start after correction of hypokalaemia and any coexisting hypomagnesaemia. Thiazide diuretics can precipitate new onset hypokalaemia or exacerbate pre-existing hypokalaemia. Thiazide diuretics should be administered with caution in patients with conditions involving enhanced potassium loss, for example salt losing nephropathies and prerenal (cardiogenic) impairment of kidney function. If hypokalaemia develops during hydrochlorothiazide therapy, Exforge HCT should be discontinued until stable correction of the potassium balance.
Thiazide diuretics can precipitate new onset hyponatraemia and hypochloroaemic alkalosis or exacerbate pre-existing hyponatraemia. Hyponatraemia, accompanied by neurological symptoms (nausea, progressive disorientation, apathy) has been observed. Treatment with hydrochlorothiazide should only be started after correction of pre-existing hyponatraemia. In case severe or rapid hyponatraemia develops during Exforge HCT therapy, the treatment should be discontinued until normalisation of natraemia.
All patients receiving thiazide diuretics should be periodically monitored for imbalances in electrolytes, particularly potassium, sodium and magnesium.
Renal impairment: Thiazide diuretics may precipitate azotaemia in patients with chronic kidney disease. When Exforge HCT is used in patients with renal impairment periodic monitoring of serum electrolytes (including potassium), creatinine and uric acid serum levels is recommended. Exforge HCT is contraindicated in patients with severe renal impairment, anuria or undergoing dialysis (see Contraindications).
No dose adjustment of Exforge HCT is required for patients with mild to moderate renal impairment (GFR ≥30 ml/min/1.73 m2).
Renal artery stenosis: Exforge HCT should be used with caution to treat hypertension in patients with unilateral or bilateral renal artery stenosis or stenosis to a solitary kidney since blood urea and serum creatinine may increase in such patients.
Kidney transplantation: To date there is no experience of the safe use of Exforge HCT in patients who have had a recent kidney transplantation.
Hepatic impairment: Valsartan is mostly eliminated unchanged via the bile. The half life of amlodipine is prolonged and AUC values are higher in patients with impaired liver function; dose recommendations have not been established. In patients with mild to moderate hepatic impairment without cholestasis, the maximum recommended dose is 80 mg valsartan, and therefore, Exforge HCT is not suitable in this group of patients (see Dosage & Administration, Contraindications and Pharmacology: Pharmacokinetics under Actions).
Angioedema: Angioedema, including swelling of the larynx and glottis, causing airway obstruction and/or swelling of the face, lips, pharynx, and/or tongue, has been reported in patients treated with valsartan. Some of these patients previously experienced angioedema with other medicinal products including ACE inhibitors. Exforge HCT should be discontinued immediately in patients who develop angioedema and should not be re-administered.
Heart failure and coronary artery disease/post-myocardial infarction: As a consequence of the inhibition of the renin-angiotensin-aldosterone system, changes in renal function may be anticipated in susceptible individuals. In patients with severe heart failure whose renal function may depend on the activity of the renin-angiotensin-aldosterone system, treatment with ACE inhibitors and angiotensin receptor antagonists has been associated with oliguria and/or progressive azotaemia and (rarely) with acute renal failure and/or death. Similar outcomes have been reported with valsartan. Evaluation of patients with heart failure or post-myocardial infarction should always include assessment of renal function.
In a long-term, placebo-controlled study (PRAISE-2) of amlodipine in patients with NYHA (New York Heart Association Classification) III and IV heart failure of non-ischaemic aetiology, amlodipine was associated with increased reports of pulmonary oedema despite no significant difference in the incidence of worsening heart failure as compared to placebo.
Calcium channel blockers, including amlodipine, should be used with caution in patients with congestive heart failure, as they may increase the risk of future cardiovascular events and mortality.
Caution is advised in patients with heart failure and coronary artery disease, particularly at the maximum dose of Exforge HCT, 10 mg/320 mg/25 mg, since available data in these patient populations is limited.
Aortic and mitral valve stenosis: As with all other vasodilators, special caution is indicated in patients with mitral stenosis or significant aortic stenosis that is not high grade.
Primary hyperaldosteronism: Patients with primary hyperaldosteronism should not be treated with the angiotensin II antagonist valsartan as their renin-angiotensin system is not activated. Therefore, Exforge HCT is not recommended in this population.
Systemic lupus erythematosus: Thiazide diuretics, including hydrochlorothiazide, have been reported to exacerbate or activate systemic lupus erythematosus.
Other metabolic disturbances: Thiazide diuretics, including hydrochlorothiazide, may alter glucose tolerance and raise serum levels of cholesterol, triglycerides and uric acid. In diabetic patients dosage adjustments of insulin or oral hypoglycaemic agents may be required.
Due to the hydrochlorothiazide component, Exforge HCT is contraindicated in symptomatic hyperuricaemia. Hydrochlorothiazide may raise the serum uric acid level due to reduced clearance of uric acid and may cause or exacerbate hyperuricaemia as well as precipitate gout in susceptible patients.
Thiazides reduce urinary calcium excretion and may cause intermittant and slight elevation of serum calcium in the absence of known disorders of calcium metabolism. Exforge HCT is contraindicated in patients with hypercalcaemia and should only be used after correction of any pre-existing hypercalcaemia. Exforge HCT should be discontinued if hypercalcaemia develops during treatment. Serum levels of calcium should be periodically monitored during treatment with thiazides. Marked hypercalcaemia may be evidence of hidden hyperparathyroidism. Thiazides should be discontinued before carrying out tests for parathyroid function.
Photosensitivity: Cases of photosensitivity reactions have been reported with thiazide diuretics (see Adverse Reactions). If photosensitivity reaction occurs during treatment with Exforge HCT, it is recommended to stop the treatment. If a readministration of the diuretic is deemed necessary, it is recommended to protect exposed areas to the sun or to artificial UVA.
Choroidal
effusion, acute myopia and secondary acute angle-closure glaucoma: Hydrochlorothiazide, a sulphonamide, has been associated with an idiosyncratic reaction resulting in choroidal effusion
with visual field defect, acute transient myopia and acute angle-closure glaucoma. Symptoms include acute onset of decreased visual acuity or ocular pain and typically occur within hours to a week of treatment initiation. Untreated acute-angle closure glaucoma can lead to permanent vision loss.
The primary treatment is to discontinue hydrochlorothiazide as rapidly as possible. Prompt medical or surgical treatment may need to be considered if the intraocular pressure remains uncontrolled. Risk factors for developing acute angle closure glaucoma may include a history of sulphonamide or penicillin allergy.
General: Caution should be exercised in patients who have shown prior hypersensitivity to other angiotensin II receptor antagonists. Hypersensitivity reactions to hydrochlorothiazide are more likely in patients with allergy and asthma.
Dual blockade of the renin-angiotensin-aldosterone system (RAAS): There is evidence that the concomitant use of ACE inhibitors, ARBs or aliskiren increases the risk of hypotension, hyperkalaemia and decreased renal function (including acute renal failure). Dual blockade of RAAS through the combined use of ACE inhibitors, ARBs or aliskiren is therefore not recommended. (See Interactions and Pharmacology: Pharmacodynamics under Actions.)
If dual blockade therapy is considered absolutely necessary, this should only occur under specialist supervision and subject to frequent close monitoring of renal function, electrolytes and blood pressure. ACE inhibitors and ARBs should not be used concomitantly in patients with diabetic nephropathy.
Non-melanoma skin cancer: An increased risk of non-melanoma skin cancer (NMSC) [basal cell carcinoma (BCC) and squamous cell carcinoma (SCC)] with increasing cumulative dose of hydrochlorothiazide exposure has been observed in two epidemiological studies based on the Danish National Cancer Registry. Photosensitising actions of hydrochlorothiazide could act as a possible mechanism for NMSC.
Patients taking hydrochlorothiazide should be informed of the risk of NMSC and advised to regularly check their skin for any new lesions and promptly report any suspicious skin lesions. Possible preventive measures such as limited exposure to sunlight and UV rays and, in case of exposure, adequate protection should be advised to the patients in order to minimise the risk of skin cancer. Suspicious skin lesions should be promptly examined potentially including histological examinations of biopsies. The use of hydrochlorothiazide may also need to be reconsidered in patients who have experienced previous NMSC (see also Adverse Reactions).
Use in the Elderly (age 65 years or over): Caution, including more frequent monitoring of blood pressure, is recommended in elderly patients, particularly at the maximum dose of Exforge HCT, 10 mg/320 mg/25 mg, since available data in this patient population are limited.
Use in Pregnancy: Angiotensin II Receptor Antagonists (AIIRAs) should not be initiated during pregnancy. Unless continued AIIRA therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with AIIRAs should be stopped immediately, and, if appropriate, alternative therapy should be started (see Contraindications and Use in Pregnancy & Lactation).
Effects on ability to drive and use machines: Patients taking Exforge HCT and driving vehicles or using machines should take into account that dizziness or weariness may occasionally occur.
Amlodipine can have mild or moderate influence on the ability to drive and use machines. If patients taking amlodipine suffer from dizziness, headache, fatigue or nausea the ability to react may be impaired.
Pregnancy: Amlodipine: The safety of amlodipine in human pregnancy has not been established. In animal studies, reproductive toxicity was observed at high doses (see Pharmacology: Toxicology: Preclinical safety data under Actions). Use in pregnancy is only recommended when there is no safer alternative and when the disease itself carries greater risk for the mother and foetus.
Valsartan: The use of Angiotensin II Receptor Antagonists (AIIRAs) is not recommended during the first trimester of pregnancy (see Precautions). The use of AIIRAs is contraindicated during the second and third trimesters of pregnancy (see Contraindications and Precautions).
Epidemiological evidence regarding the risk of teratogenicity following exposure to ACE inhibitors during the first trimester of pregnancy has not been conclusive; however a small increase in risk cannot be excluded. Whilst there is no controlled epidemiological data on the risk with Angiotensin II Receptor Antagonists (AIIRAs), similar risks may exist for this class of drugs. Unless continued AIIRA therapy is considered essential, patients planning pregnancy should be changed to alternative antihypertensive treatments which have an established safety profile for use in pregnancy. When pregnancy is diagnosed, treatment with AIIRAs should be stopped immediately, and if appropriate, alternative therapy should be started.
Exposure to AIIRAs therapy during the second and third trimesters is known to induce human foetotoxicity (decreased renal function, oligohydramnios, skull ossification retardation) and neonatal toxicity (renal failure, hypotension, hyperkalaemia) (see Pharmacology: Toxicology: Preclinical safety data under Actions).
Should exposure to AIIRAs have occurred from the second trimester of pregnancy, ultrasound check of renal function and skull is recommended.
Infants whose mothers have taken AIIRAs should be closely observed for hypotension (see Contraindications and Precautions).
Hydrochlorothiazide: There is limited experience with hydrochlorothiazide during pregnancy, especially during the first trimester. Animal studies are insufficient.
Hydrochlorothiazide crosses the placenta. Based on the pharmacological mechanism of action of hydrochlorothiazide, its use during the second and third trimester may compromise foeto-placental perfusion and may cause foetal and neonatal effects like icterus, disturbance of electrolyte balance and thrombocytopenia.
Amlodipine/valsartan/hydrochlorothiazide: There is no experience on the use of Exforge HCT in pregnant women. Based on the existing data with the components, the use of Exforge HCT is not recommended during first trimester and contra-indicated during the second and third trimester of pregnancy (see Contraindications and Precautions).
Breast-feeding: Amlodipine is excreted in human milk. The proportion of the maternal dose received by the infant has been estimated with an interquartile range of 3-7%, with a maximum of 15%. The effect of amlodipine on infants is unknown. No information is available regarding the use of valsartan during breast-feeding. Hydrochlorothiazide is excreted in human milk in small amounts. Thiazides in high doses causing intense diuresis can inhibit milk production. The use of Exforge HCT during breast-feeding is not recommended. If Exforge HCT is used during breast-feeding, doses should be kept as low as possible. Alternative treatments with better established safety profiles during breast-feeding are preferable, especially while nursing a newborn or preterm infant.
Fertility: There are no clinical studies on fertility with Exforge HCT.
Valsartan: Valsartan had no adverse effects on the reproductive performance of male or female rats at oral doses up to 200 mg/kg/day. This dose is 6 times the maximum recommended human dose on a mg/m2 basis (calculations assume an oral dose of 320 mg/day and a 60-kg patient).
Amlodipine: Reversible biochemical changes in the head of spermatozoa have been reported in some patients treated by calcium channel blockers. Clinical data are insufficient regarding the potential effect of amlodipine on fertility. In one rat study, adverse effects were found on male fertility (see Pharmacology: Toxicology: Preclinical safety data under Actions).
The safety profile of Exforge HCT presented below is based on clinical studies performed with Exforge HCT and the known safety profile of the individual components amlodipine, valsartan and hydrochlorothiazide.
Summary of the safety profile: The safety of Exforge HCT has been evaluated at its maximum dose of 10 mg/320 mg/25 mg in one controlled short-term (8 weeks) clinical study with 2,271 patients, 582 of whom received valsartan in combination with amlodipine and hydrochlorothiazide. Adverse reactions were generally mild and transient in nature and only infrequently required discontinuation of therapy. In this active controlled clinical trial, the most common reasons for discontinuation of therapy with Exforge HCT were dizziness and hypotension (0.7%).
In the 8-week controlled clinical study, no significant new or unexpected adverse reactions were observed with triple therapy treatment compared to the known effects of the monotherapy or dual therapy components.
In the 8-week controlled clinical study, changes in laboratory parameters observed with the combination of Exforge HCT were minor and consistent with the pharmacological mechanism of action of the monotherapy agents. The presence of valsartan in the triple combination attenuated the hypokalaemic effect of hydrochlorothiazide.
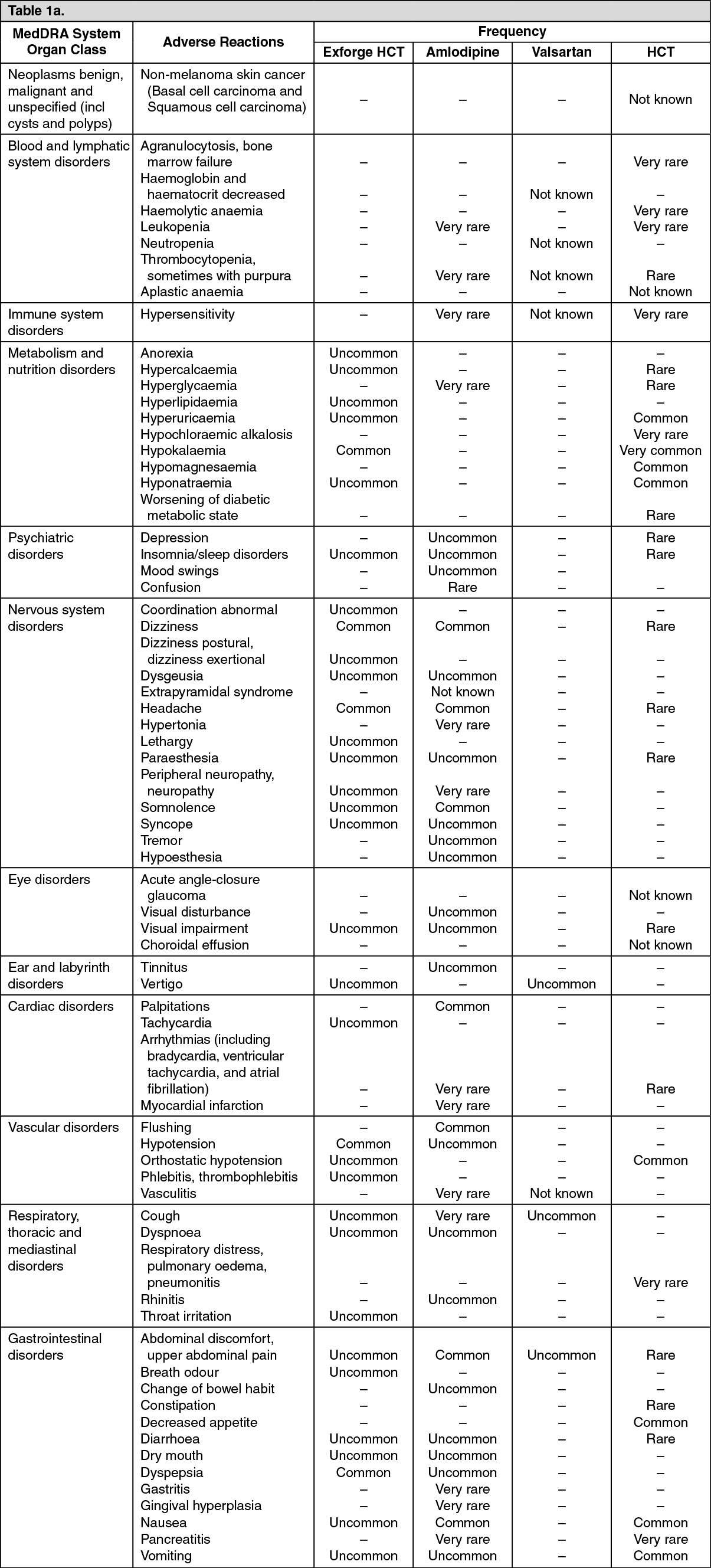
Tabulated list of adverse reactions: The following adverse reactions, listed by MedDRA System Organ Class and frequency, concern Exforge HCT (amlodipine/valsartan/HCT) and amlodipine, valsartan and HCT individually.
Very common: ≥1/10; common: ≥1/100 to <1/10; uncommon: ≥1/1,000 to <1/100; rare: ≥1/10,000 to <1/1,000; very rare: <1/10,000, not known (cannot be estimated from the available data). (See Tables 1a and 1b.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Description of selected adverse reactions: Non-melanoma skin cancer:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Description of selected adverse reactions: Non-melanoma skin cancer: based on available data from epidemiological studies, cumulative dose-dependent association between hydrochlorothiazide and NMSC has been observed (see also Precautions and Pharmacology: Pharmacodynamics under Actions).
Reporting of suspected adverse reactions: Reporting suspected adverse reactions after authorisation of the medicinal product is important. It allows continued monitoring of the benefit/risk balance of the medicinal product. Healthcare professionals are asked to report any suspected adverse reactions.
No formal interaction studies with other medicinal products have been performed with Exforge HCT. Thus, only information on interactions with other medicinal products that are known for the individual active substances is provided in this section.
However, it is important to take into account that Exforge HCT may increase the hypotensive effect of other antihypertensive agents.
See Tables 2a and 2b.
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Dual blockade of the RAAS with ARBs, ACE inhibitors or aliskiren: Clinical trial data have shown that dual blockade of the RAAS through the combined use of ACE inhibitors, ARBs or aliskiren is associated with a higher frequency of adverse events such as hypotension, hyperkalaemia and decreased renal function (including acute renal failure) compared to the use of a single RAAS-acting agent (see Contraindications, Precautions and Pharmacology: Pharmacodynamics under Actions).
Incompatibilities: Not applicable.
C09DX01 - valsartan, amlodipine and hydrochlorothiazide ; Belongs to the class of angiotensin II receptor blockers (ARBs), other combinations. Used in the treatment of cardiovascular disease.
Exforge HCT 10/160/12.5 mg fim-coated tab
28's
Exforge HCT 10/160/25 mg film-coated tab
28's
Exforge HCT 5/160/12.5 mg film-coated tab
28's


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image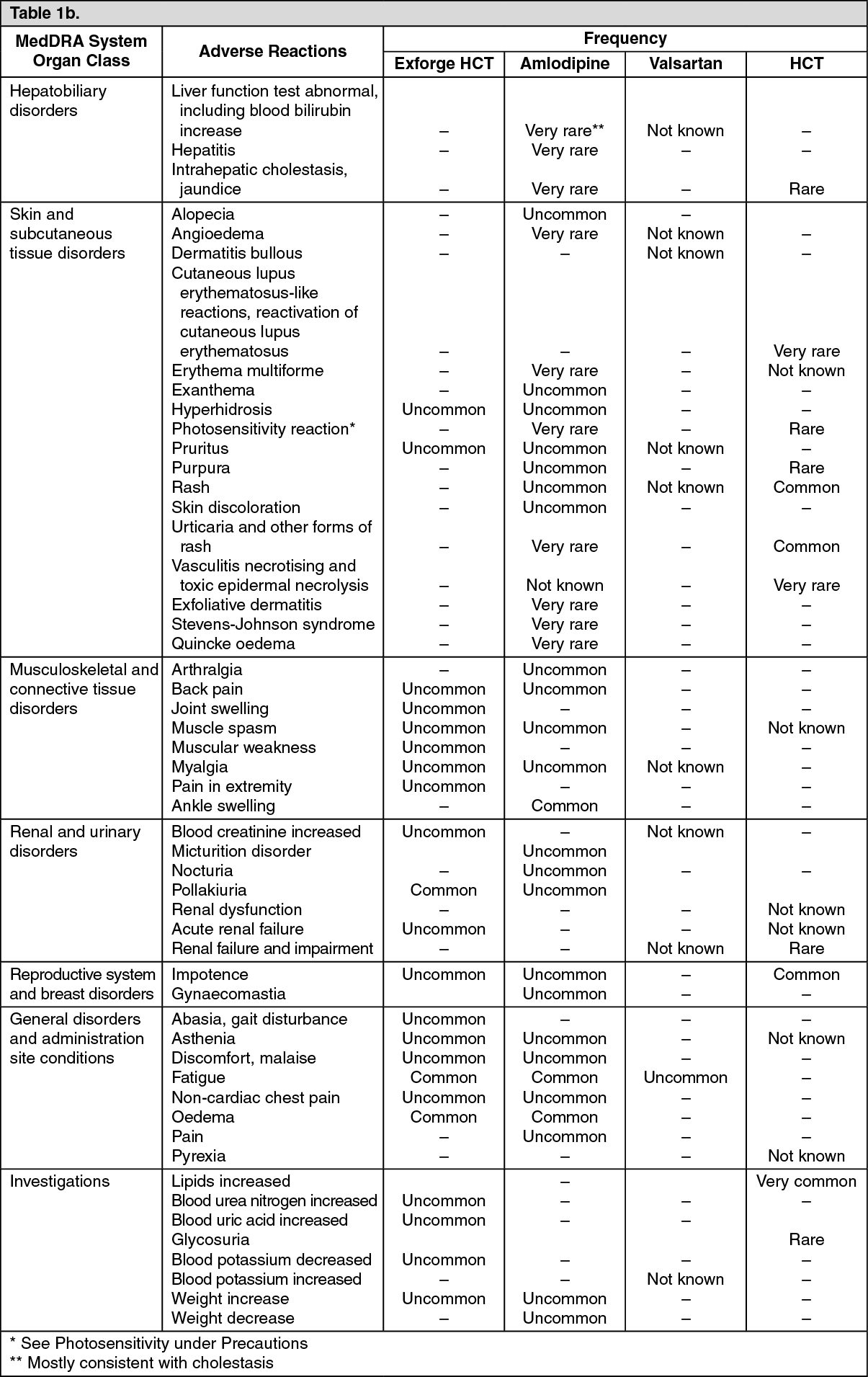 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image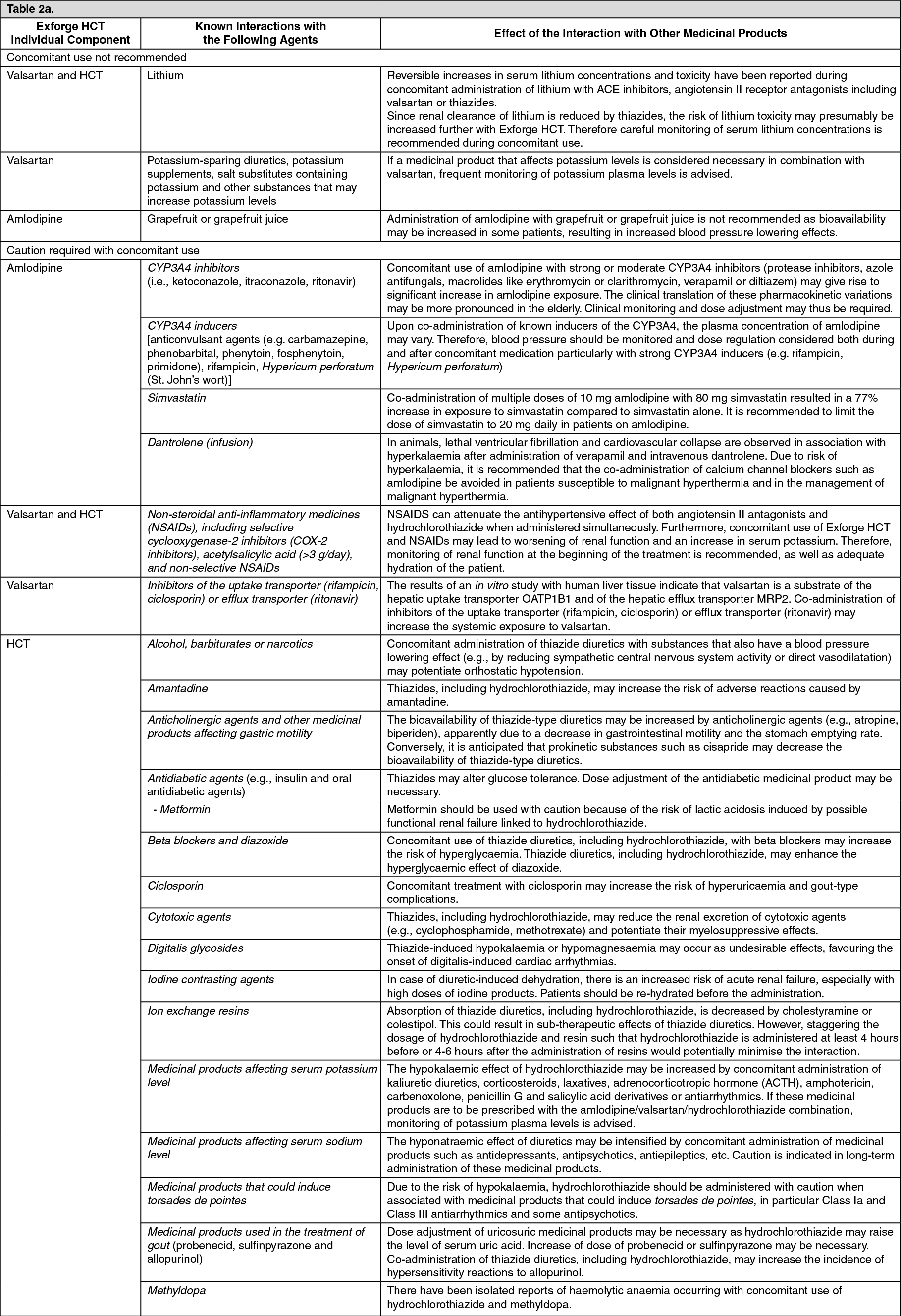 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image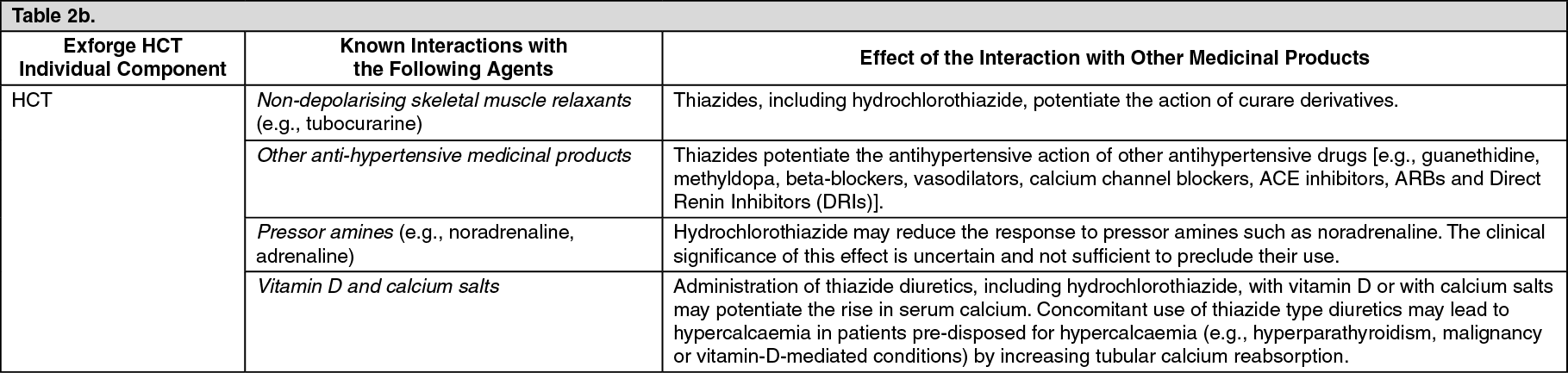 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
